THE DEFINITIVE GUIDE FOR THE TREATMENT OF DYSMENORRHOEA
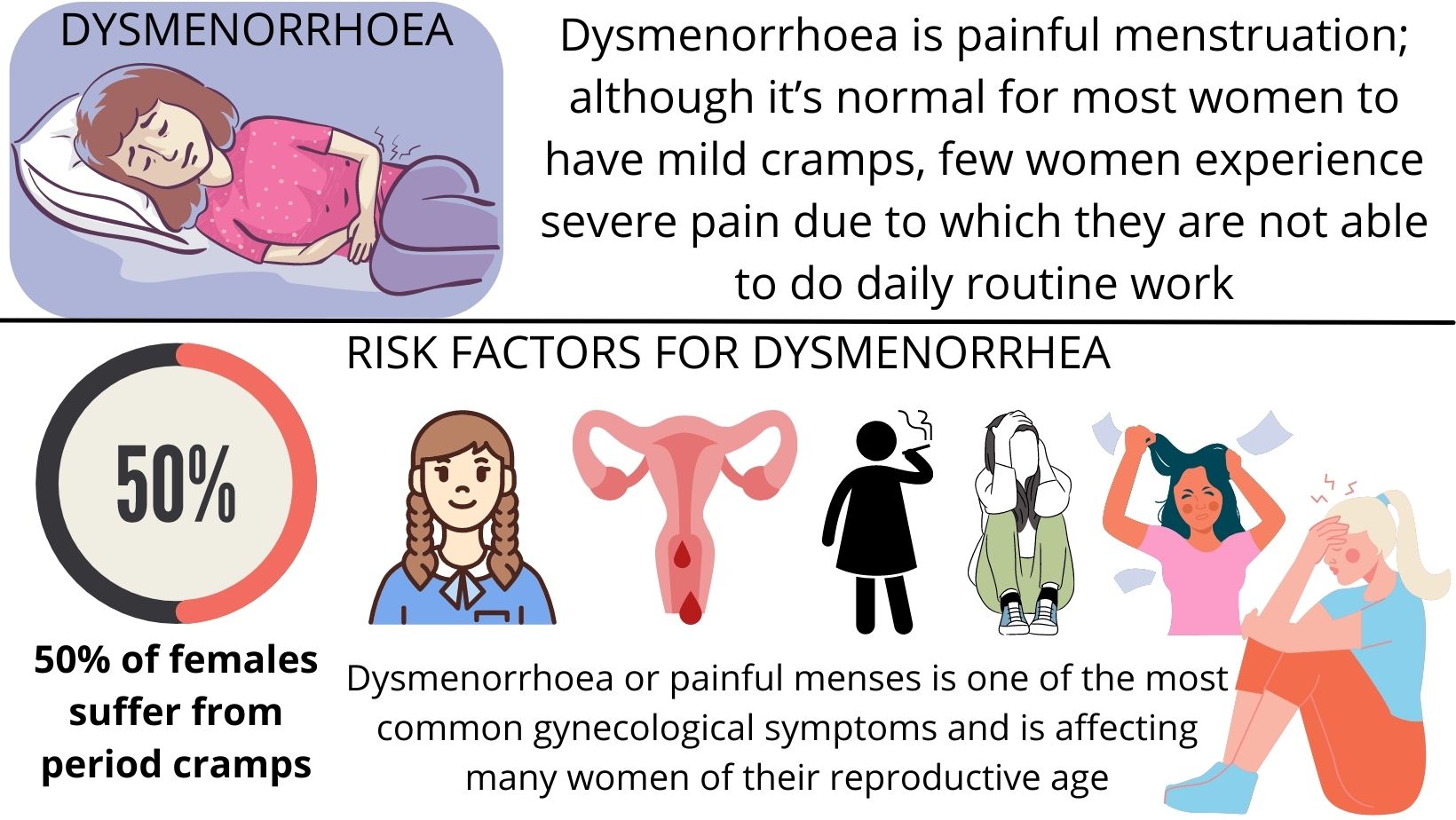
WHAT IS DYSMENORRHOEA?
WHAT ARE THE RISK FACTORS FOR DYSMENORRHEA
- Young age
- early menarche
- heavy menstrual flow
- nulliparity (a state in which a woman has never carried a pregnancy)
- smoking
- depression
- anxiety
- stress
WHAT ARE THE TYPES OF DYSMENORRHOEA?
PRIMARY (no pathology)- primary dysmenorrhoea is the presence of painful menses in absence of any pathology.
Primary dysmenorrhoea is caused by excessive levels of prostaglandins (hormones that cause contraction of the uterus). it affects adolescent girls but the problem ceases as they mature, particularly after a pregnancy.
- vaginal discharge
- dyspareunia (painful sexual intercourse)
- menorrhagia (heavy bleeding at menstruation).
- fibroid
- adenomyosis
- sexually transmitted infection
- endometriosis
- pelvic inflammatory disease
- ovarian cyst
- intrauterine device.
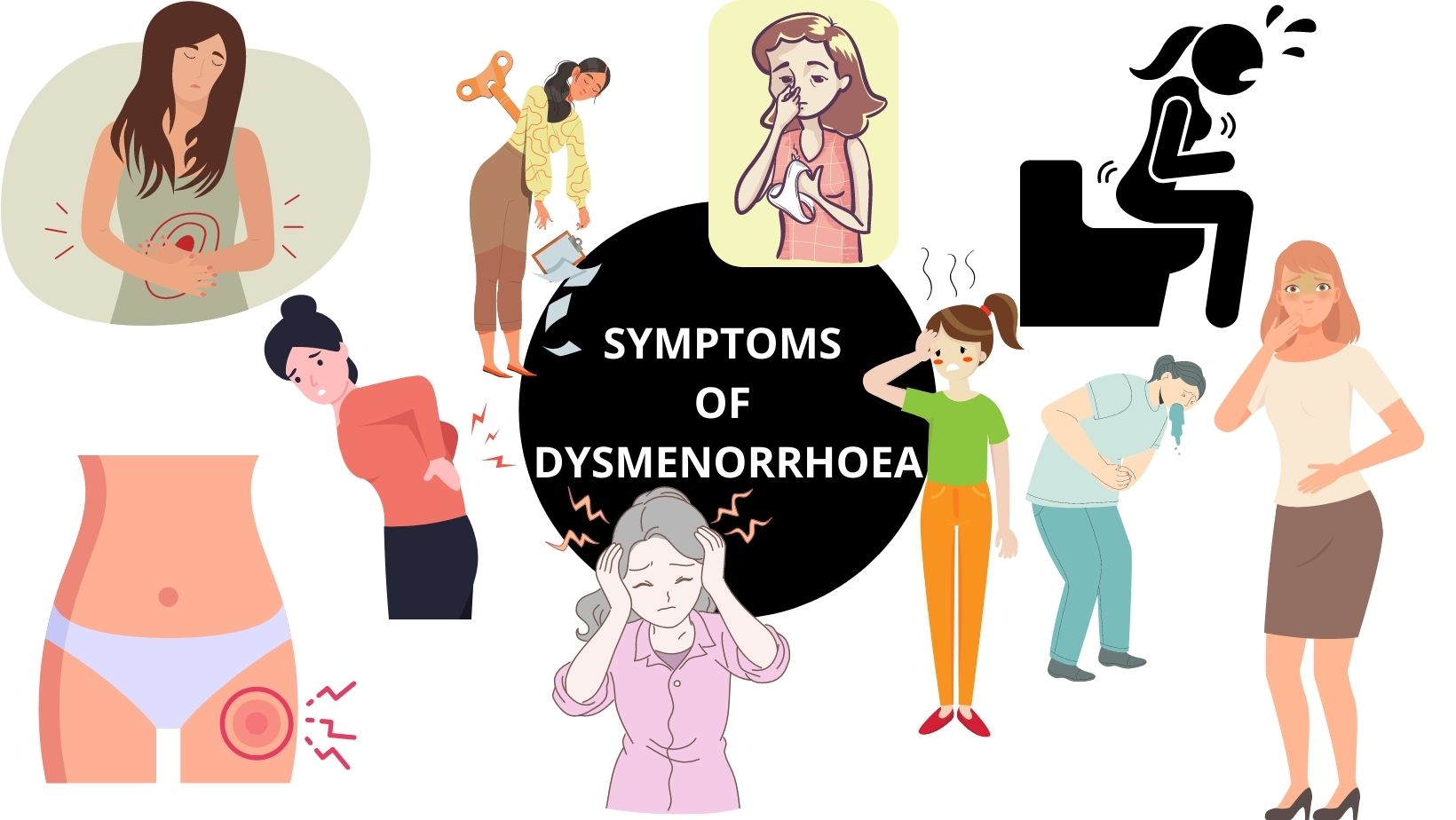
WHAT ARE THE SYMPTOMS OF DYSMENORRHOEA?
WHAT ARE THE CAUSES OF DYSMENORRHOEA?
- Endometriosis
- Pelvic Inflammatory Disease ( Infections)
- Adenomyosis
- Intrauterine polyps
- Submucosal fibroids
- IUCDs
- Congenital uterine abnormalities
- Cervical stenosis
- Asherman syndrome
- Chronic ectopic pregnancy
- Pelvic congestion syndrome
- Ovarian cysts or neoplasms
DIAGNOSIS OF DYSMENORRHOEA
- History taking and physical examination along with pelvic examination would diagnose the case.
- A transvaginal ultrasound should be performed if secondary dysmenorrhoea is suspected.
TREATMENT OF DYSMENORRHOEA
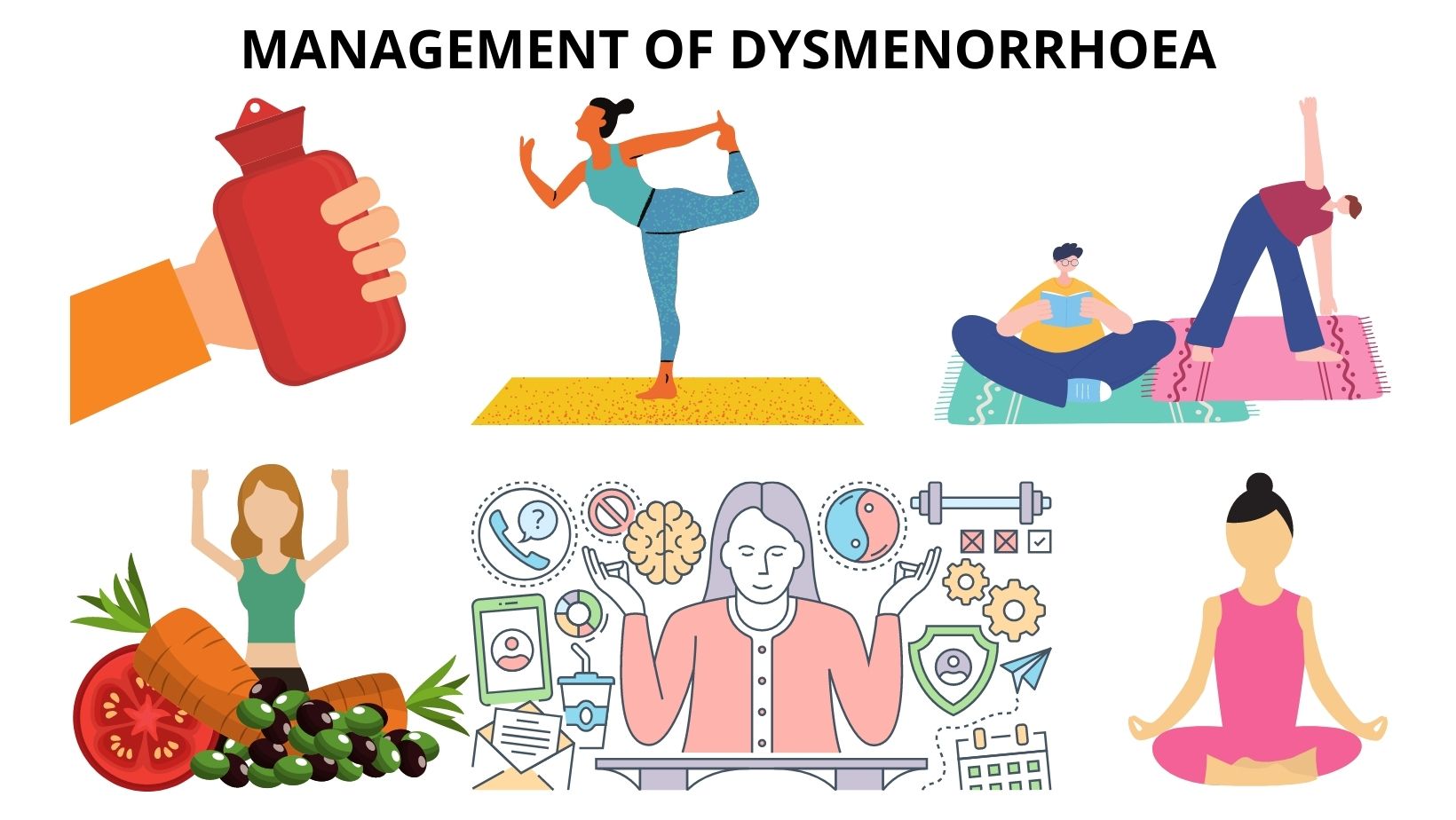
MANAGEMENT OF DYSMENORRHOEA
-
Pain management is very important.
-
Ask the patient to stay active and do regular physical exercise.
-
The patient should be advised to do yoga.
-
Advice patient to use a hot water bottle for fomentation during pain.
-
The patient should be advised to take a healthy diet.
HOMEOPATHIC MANAGEMENT OF DYSMENORRHOEA
DO’S AND DON’TS
DO’S
- Regular exercise.
- Yoga
- Healthy diet.
- Healthy lifestyle
DON’TS
- Manage anxiety/ stress
- Quit Smoking.
- Don't take Alcohol
Get Free Consultation
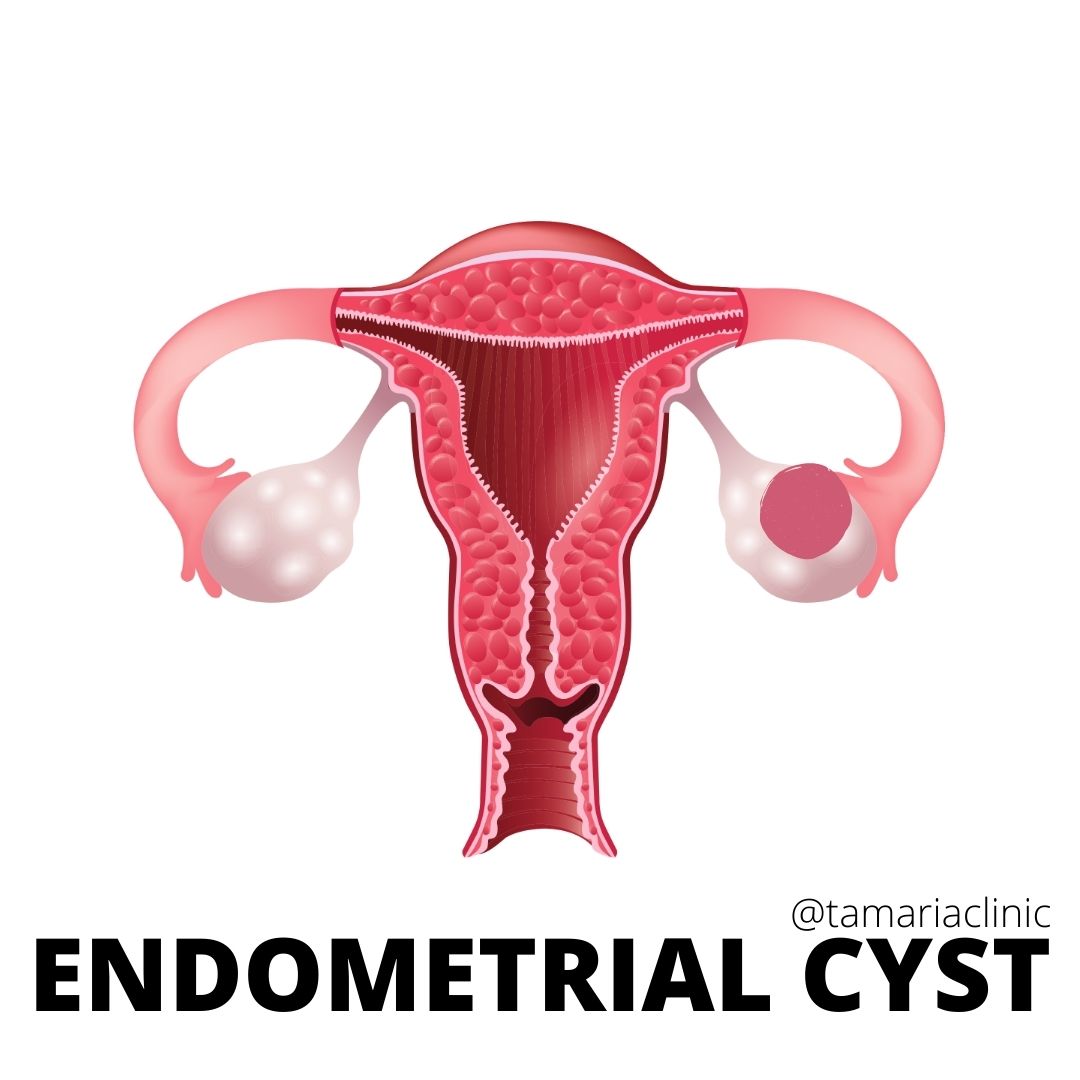
ALL YOU NEED TO KNOW ABOUT ENDOMETRIAL CYSTS!!
When the endometrial cells get to the ovaries, they form cysts or lumps and the size may vary from less than 2” up to 8”.
HEADACHE VERSUS MIGRAINE!!
Differentiation obviously can help in better management and treatment as headaches could be a symptom of an illness however migraine itself is an illness.
10 SIGNS YOU MIGHT BE SUFFERING FROM HYPOTHYROIDISM
The thyroid gland controls energy balance thus tiredness is the most common sign to go for hypothyroidism
7 WARNING SIGNS TO LOOK FOR GOUT
Gout is a form of arthritis characterized by sudden, severe attacks of pain, swelling, redness, and tenderness of one or more joints
Comments
We have received your comment , Thank You !